
Virus Watch preliminary findings on 16th Dec 2024
Virus Watch is a research study run by University College London and the NHS. The study aims to identify how COVID-19 spreads, and how to stop it. Findings so far presented on this page are early, preliminary results and should be interpreted with caution as they have not all yet been peer-reviewed by scientists external to our research collaborators. We are presenting these early findings to participants, the general public and policy makers. A detailed description of the Virus Watch study and our research questions can be found in our study protocol. Virus Watch began recruiting people in June 2020 and since then, 58,628 people in 28,527 households across England and Wales have joined the study. You can find a detailed description of the cohort in a profile of the study here.
Table of contents
- Summary of findings
- Estimating the risk of long covid in deprived communities, migrants and ethnic minorities
- Virus Watch Impacts: The Occupational Impact of COVID-19 in the UK in the Transport and Education Sectors
1. Summary of findings:
Estimating the risk of Long COVID in deprived communities, migrants and ethnic minorities.
- The link between social characteristics and people’s likelihood of developing Long Covid is not well understood, especially in later periods of the pandemic when different COVID variants were circulating.
- We investigated how deprivation, migration status and ethnic minority status affect the likelihood of developing long COVID in all individuals regardless of whether they had ever been infected with COVID-19 and in those with a confirmed COVID-19 infection. This can give us an indication of whether the factors that may lead to long COVID come from before or after getting infected.
- During the pre-Omicron period, more deprived populations were more likely to develop long COVID, especially among females. Migrant, ethnic minority and migrant-ethnic minority males were also more likely to develop long COVID compared to their counterparts.
- In the Omicron period, the disparities in the likelihood of long COVID were less pronounced, though migrant-ethnic minority females still had a higher long COVID probability, especially in those with confirmed infections.
- Our study suggests pre- and post-infection factors influenced the probability of long COVID among these populations and highlights the need to address health inequalities faced by them to reduce their risk of COVID-19 infection and long COVID.
Virus Watch Impacts: The Occupational Impact of COVID-19 in the UK in the Transport and Education Sectors
The Virus Watch team conducted analyses investigating how people’s jobsimpacted their risk of catching Covid-19. We also investigated how exposure at work differed depending on people’s jobs and what kind of mitigation methods to reduce exposure were used in workplaces.
We found that frontline transport workers had 2.2x times the odds of being positive for COVID-19 during the early pandemic compared with professional occupations that could work primarily from home. We also showed that exposure at work was an important part of these increased odds of infection.
Other studies looked at hospitalisations and deaths, and found that public-facing transport workers were more likely to have severe COVID-19 outcomes compared to people who could work remotely.
These findings have been included in a report recommending that public-facing transport workers are now eligible for industrial injury compensation following severe complications of COVID-19. This has now been presented to parliament by the Secretary of State for Work and Pensions.
- Preliminary findings November 2020
- Preliminary findings January 2021
- Preliminary findings March 2021
- Preliminary findings May 2021
- Preliminary findings June 2021
- Preliminary findings December 2021
- Preliminary findings February 2022
- Preliminary findings December 2022
- Preliminary findings July 2023
- Preliminary findings December 2023
- Preliminary findings July 2024
You can also find a list of our publications here.
2. Estimating the risk of long covid in deprived communities, migrants and ethnic minorities.
Read the full analysis here: https://www.medrxiv.org/content/10.1101/2024.11.26.24317965v2
Deprived communities, migrant and ethnic minorities were disproportionately affected by COVID-19 and may therefore be at a higher risk of long COVID. We aimed to investigate how deprivation, migration status and ethnic minority status affect the likelihood of developing long COVID. We assessed the risk in all individuals regardless of whether they had ever been infected with COVID-19 (full cohort) and in those with a confirmed COVID-19 infection (confirmed cohort). This can give us an indication of whether the factors that may lead to long COVID come from before or after getting infected.
When wild-type, Alpha, and Delta variants were circulating, people living in more deprived neighbourhoods were more likely to develop long COVID, especially among females. At the same time, males from migrant, ethnic minority and migrant-ethnic minority backgrounds were also more likely to develop long COVID than their counterparts.
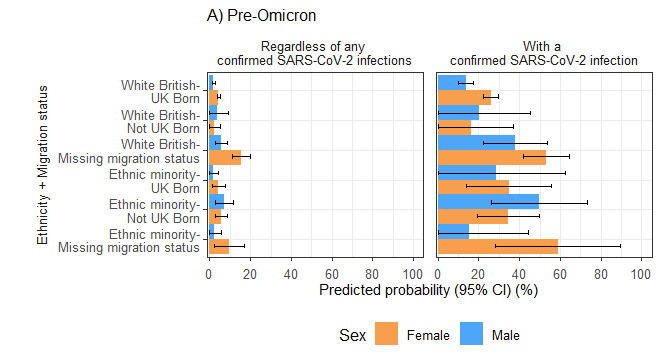
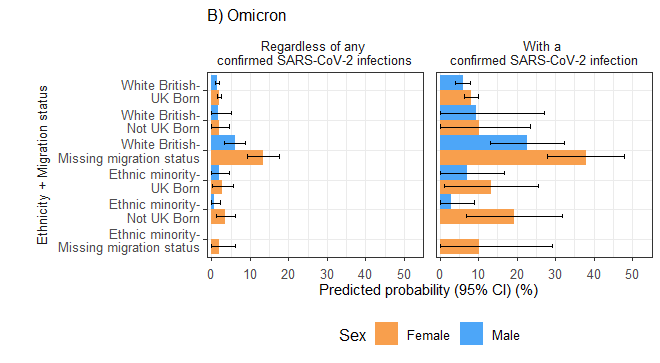
In the Omicron period, the differences in the likelihood of long COVID were less pronounced. However, females from migrant-ethnic minority backgrounds were still more likely to develop long COVID. Amongst females with a confirmed COVID infection, 19.4% of ethnic minority migrant females developed Long Covid compared to 8.2% of white British UK-born females.
Higher probabilities of long COVID among migrants, ethnic minorities and deprived populations during the pre-Omicron period than the Omicron period reflect intervention-induced inequalities during the pre-Omicron period. Measures including lockdowns, work-from-home policies and access to vaccines lowered overall infection rates but had differential impact across these populations depending on work-related and housing-related exposures. By the Omicron period, once restrictions were lifted, the observed inequality gaps in our analysis narrowed when infection became more widespread.
Our findings also suggest that the greater likelihood of developing long Covid among migrants, ethnic minorities and deprived populations is driven by both increased infection risk and post-infection factors, which highlights the critical need to tackle health inequalities to minimise the infection risk and long-term consequences from COVID-19 and future pandemics, especially for these populations.
Figure 1. Predicted probabilities of Long Covid by IMD quintile, migration status and ethnic minority status in the full cohort and individuals with a previous SARS-CoV-2 infection, categorised by reported sex-at-birth during A) pre-Omicron and B) Omicron periods.
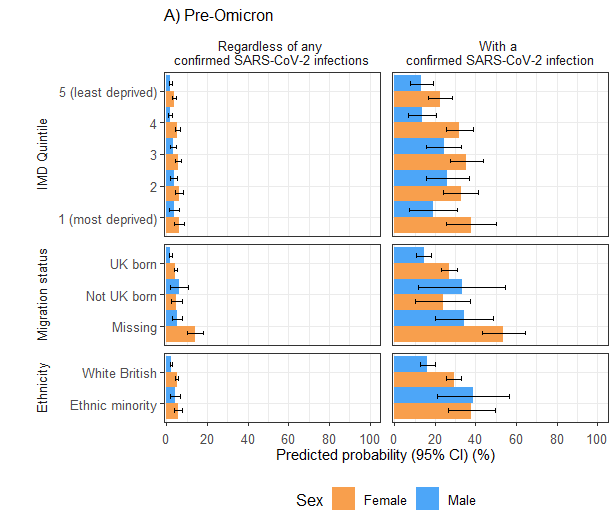
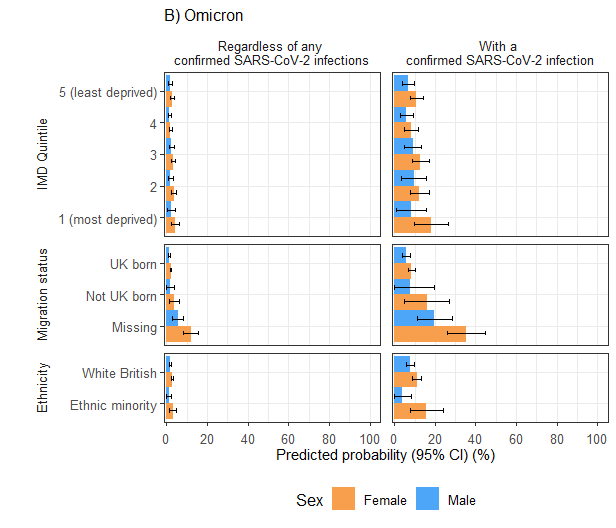
Figure 2. Predicted probability of Long Covid by the ‘ethnicity-migration’ composite variable in the full cohort and individuals with a previous SARS-CoV-2 infection, stratified by reported sex-at-birth during A) pre-Omicron and B) Omicron periods. No PP/OR estimates available for males in the ‘ethnic minority-missing migration status’ group from the Omicron period due to small sample size.
3. Virus Watch Policy Impacts: The Occupational Impact of COVID-19 in the UK in the Transport and Education Sectors
Background
- The Virus Watch team conducted analyses investigating how people’s jobs impacted their risk of catching Covid-19. We also investigated how exposure at work differed depending on people’s jobs and what kind of mitigation methods to reduce exposure were used in workplaces (1, 2)
- We worked with other researchers who examined severe outcomes from other data sources such as hospitalisations and deaths as part of a national project called PROTECT (Partnership for Research in Occupational, Transport and Environmental COVID Transmission) (https://sites.manchester.ac.uk/covid19-national-project/)
- We found that frontline transport workers had 2.2x times the odds of being positive for COVID-19 during the early pandemic compared with professional occupations that could work primarily from home. We also showed that exposure at work was an important part of these increased odds of infection (1)
- Other studies looked at hospitalisations and deaths, and found that public-facing transport workers were more likely to have severe COVID-19 outcomes compared to people who could work remotely (3)

Report
- The Industrial Injuries Advisory Council are a scientific body that advise the government about workplace health and safety and industrial injury benefits
- They have produced a report recommending that public-facing transport workers are now eligible for industrial injury compensation following severe complications of COVID-19 (3). This has now been presented to parliament by the Secretary of State for Work and Pensions
- Previously, only health and social care workers were eligible for similar compensation
- The council also looked at risk in education workers, but there was not enough consistent evidence to make a recommendation
- The council recognises that other occupations may also be at risk, but are still investigating the evidence
Implications
- This is a step forward in terms of recognising the risk to public-facing workers – such as transport workers – from pandemic viral infections such as COVID-19
- Virus Watch participants have played an important role in generating this evidence
References
1. Beale S et al. Occupation, work-related contact and SARS-CoV-2 anti-nucleocapsid serological status: findings from the Virus Watch prospective cohort study. OEM 2022, doi:10.1136/oemed-2021-107920
2. Beale S, Yavlinsky A, Hoskins S et al. Between-occupation differences in work-related COVID-19 mitigation strategies over time: Analysis of the Virus Watch Cohort in England and Wales. Scand J Work Environ Health 2023b;49(5):350-362.
3. Industrial Injuries Advisory Council . The Occupational Impact of COVID-19 in the Transport and Education Sectors. https://assets.publishing.service.gov.uk/media/6735c0a554652d03d51610ec/occ-imp-covid-19-transport-educationa.pdf