
Virus Watch preliminary findings on 20 Dec 2022
You can find our most recent results at findings so far.
Virus Watch is a research study run by University College London and the NHS. The study aims to identify how COVID-19 spreads, and how to stop it. Findings so far presented on this page are early, preliminary results and should be interpreted with caution as they have not yet been peer-reviewed by scientists external to our research collaborators. We are presenting these early findings for participants, the general public and policy makers. A detailed description of the Virus Watch study and our research questions can be found in our study protocol. Virus Watch began recruiting people in June 2020 and since then, 58,628 people in 28,527 households across England and Wales have joined the study.
Table of contents
- Summary of findings
- Profile of the Virus Watch cohort
- Occupational differences in the usage of work-related mitigations against SARs-CoV-2 and workers’ perceptions of these mitigations
- Glasses and risk of COVID-19 transmission
1. Summary of findings:
Profile of the Virus Watch cohort
- A total of 58,628 volunteers in 28,527 households have agreed take part in the Virus Watch study.
- In the first 6 months of the study, approximately 75% of enrolled participants were regularly completing the weekly illness surveys.
- As of 7th December 2022, 1,619,300 weekly surveys had been submitted by Virus Watch participants with 21,299,348 person days of follow up, and 351,751 individual responses to monthly surveys received.
- Data collected include details on occupation, co-morbidities (other illnesses or conditions that participants have), medications that people use, and infection-prevention behaviours (such as hand washing and mask wearing).
- Our monthly surveys have captured information about household finance, employment, mental health, access to healthcare, vaccination uptake, long COVID and activities and contacts.
- We have conducted two laboratory substudies where we collected 10,974 full serological samples, 107,708 finger prick samples to test for the presence and the level of antibodies at different times during the pandemic (pre and post vaccine). Live virus neutralisation activity was tested in almost 5000 samples.
Occupational differences in the usage of work-related mitigations against SARs-CoV-2 and workers’ perceptions of these mitigations
- We examined differences in the usage of work-related mitigation to prevent the spread of disease as no studies have been undertaken to examine how they were applied across different phases of the pandemic and in different occupational settings.
- A survey covering the periods of late December 2020–February 2022 was developed and disseminated online to employed or self-employed participants in the Virus Watch study (n=6,279 respondents).
- We found that usage of work-related mitigation methods differed between occupations and over time, likely reflecting variation in job roles, workplace environments, legislation and guidance.
- Across all occupations greater than 50% of participants agreed or strongly agreed with each measure except physical distancing.
- Further investigation into the factors underlying between-occupational differences could assist pandemic planning and prevention of workplace COVID-19 transmission.
Glasses and risk of COVID-19 transmission
- Respiratory viruses, including SARS-CoV-2, can infect the eyes or pass into the nose via the nasolacrimal duct. The importance of transmission via the eyes is unknown but might plausibly be reduced in those who wear glasses.
- 19,166 Virus Watch participants responded to a monthly questionnaire on glasses and contact lens use, assessing reported frequency, the purpose of use and how likely they were to wear a mask with glasses.
- We found that after we accounted for differences in age, sex, household income and occupation, there was 15% lower risk of infection for those who reported always using glasses for general use compared to those who never wore glasses.
- Our findings suggest a moderate reduction in risk of SARS-CoV-2 infection in those who always wear glasses compared to never.
You can find our previous findings on the link below.
- Preliminary findings November 2020
- Preliminary findings January 2021
- Preliminary findings March 2021
- Preliminary findings May 2021
- Preliminary findings June 2021
- Preliminary findings December 2021
- Preliminary findings February 2022
2. Profile of the Virus Watch cohort
This piece of work describes how we went about recruiting a total of 58,628 volunteers in 28,527 households to take part in the Virus Watch study and what data we have been collecting throughout the study. When people first registered for Virus Watch we collected demographic information which included the age, sex, ethnicity and region of England or Wales where participants were living (see Table 1). The Virus Watch cohort is older (mean age = 48 years), with a greater proportion of people in the 45–64 year age group when compared to the general population (34% in Virus Watch compared to 26% in the general population). Some ethnic groups are also under-represented, notably the Black and Other Asian groups (Table 1).
Table 1. Demographics of Virus Watch study participants
| Characteristic | Virus Watch Participants | ONS (%)* |
| All | 58,628 | – |
| Age group (years) | ||
| 0-15 | 7,371 (13%) | 19% |
| 16-24 | 3,499 (6.0%) | 11% |
| 25-44 | 11,725 (20%) | 26% |
| 45-64 | 19,657 (34%) | 26% |
| 65+ | 16,376 (28%) | 19% |
| Sex (self-reported)** | ||
| Male | 21,687 (37%) | 49% |
| Female | 27,506 (47%) | 51% |
| Other/Missing/Prefer not to say | 9,435 (16%) | – |
| Sex (including derived)** | ||
| Male | 26,274 (45%) | 49% |
| Female | 31,533 (54%) | 51% |
| Other/Missing/Prefer not to say | 821 (1.4%) | – |
| Ethnicity | ||
| White British | 40,481 (69%) | 81% |
| White Irish | 671 (1.1%) | 1% |
| White Other | 2,816 (4.8%) | 4% |
| Mixed | 998 (1.7%) | 2% |
| South Asian | 2,728 (4.7%) | 5% |
| Other Asian | 427 (0.7%) | 2% |
| Black | 493 (0.8%) | 3% |
| Other Ethnicity | 288 (0.5%) | 1% |
| Prefer not to say | 192 (0.3%) | – |
| Missing | 9,534 (16%) | – |
| Region | ||
| North East | 2,528 (4.3%) | 5% |
| North West | 5,572 (9.5%) | 12% |
| Yorkshire and The Humber | 3,035 (5.2%) | 9% |
| East Midlands | 4,945 (8.4%) | 8% |
| West Midlands | 3,020 (5.2%) | 10% |
| East of England | 10,545 (18%) | 11% |
| London | 9,083 (15%) | 15% |
| South East | 9,845 (17%) | 15% |
| South West | 3,956 (6.7%) | 10% |
| Wales | 1,532 (2.6%) | 5% |
| Missing | 4,567 (7.8%) | – |
** Sex at birth was self-reported. If missing, sex was obtained via data linkage or derived via name-gender matching based on US names from 1930-2015 https://data.world/howarder/gender-by-name (4)
We also detail how many people stayed in the cohort throughout the study (Figure 1). In the first 6 months of the study, approximately 75% of enrolled participants were regularly completing the weekly illness surveys (Figure 1). Over the course of the pandemic the proportion of participants who were lost to follow-up steadily increased and by May 2022 the proportion still regularly completing surveys was around 50%, which remains high for a study of this nature.
Figure 1: Recruitment and retention over time (June 2020-May 2022)

As of 7th December 2022 1,619,300 weekly surveys had been submitted by Virus Watch participants with 21,299,348 person days of follow up, and 351,751 individual responses to monthly surveys were received. Data collected include details on occupation, co-morbidities (other illnesses or conditions that participants have), medications that people use, and infection-prevention behaviours (such as hand washing and mask wearing). Households were followed up weekly with illness surveys capturing symptoms and their severity, and the activities undertaken in the week prior to symptom onset and any COVID-19 test results.
Our monthly surveys have captured information about household finance, employment, mental health, access to healthcare, vaccination uptake, long COVID and activities and contacts. Virus Watch cohort data have been linked to Hospital Episode Statistics (HES), inpatient and critical care episodes, outpatient visits, emergency care contacts, mortality, virology testing and vaccination data held by NHS Digital.
Nested within Virus Watch are several sub-studies. We have stored serum at 2 time points from 12,877 participants (adults and children) that took part in the serology & PCR subcohort, as well as longitudinal serum micro-samples from the vaccine evaluation subcohort of 19,555 adult participants. These blood samples allow us to measure antibodies and examine risk factors for infection to COVID-19 after taking into account co-morbidities, previous infection exposure and vaccination status.
A unique strength of Virus Watch is that we follow up whole households longitudinally, rather than being limited to individuals. The cohort has data on all ages including children and adolescents and is broadly representative of the UK population on geographic spread and deprivation (Table 1), with some exceptions. Virus Watch is one of the few longitudinal studies to present quantitative spike and nucleocapsid antibody test data together with detailed vaccination information and clinical comorbidities, which has enabled us to make several important discoveries about the vaccines.
The cohort has several important limitations which guided our inclusion criteria. Households self-selected into the study after receiving an invitation via multiple routes. Households with more than six members were not eligible for the study due to the limitations of the secure system we used to collect participant data. People living in institutional settings such as care homes, university halls of residence and boarding schools were not eligible to participate, limiting the generalisability of findings for these groups. Households also needed to have either a mobile telephone, tablet or computer with an internet connection, a valid email address and at least one household member who could read and respond in English to complete regular surveys.
Please see this link for the full analysis and here for the supplemental analysis.
3. Occupational differences in the usage of work-related mitigations against SARs-CoV-2 and workers’ perceptions of these mitigations.
The COVID-19 pandemic has had a profound impact on workplaces. A diverse range of mitigation methods have been employed during the COVID-19 pandemic to reduce SARS-CoV-2 transmission in workplaces. These have included workplace closures, behavioural and environmental measures to reduce transmission (e.g., testing programmes and requirements to isolate from work if infectious), and promotion of COVID-19 vaccination by employers.
In this analysis, we examined differences in the usage of work-related mitigation to prevent the spread of disease as no studies have been undertaken to examine how they were applied across different phases of the pandemic and in different occupational settings. A survey covering the periods of late December 2020–February 2022 was developed and disseminated online to employed or self-employed participants in the Virus Watch study (n=6,279 respondents).
We found that usage of work-related mitigation methods differed between occupations and over time, likely reflecting variation in job roles, workplace environments, legislation and guidance.
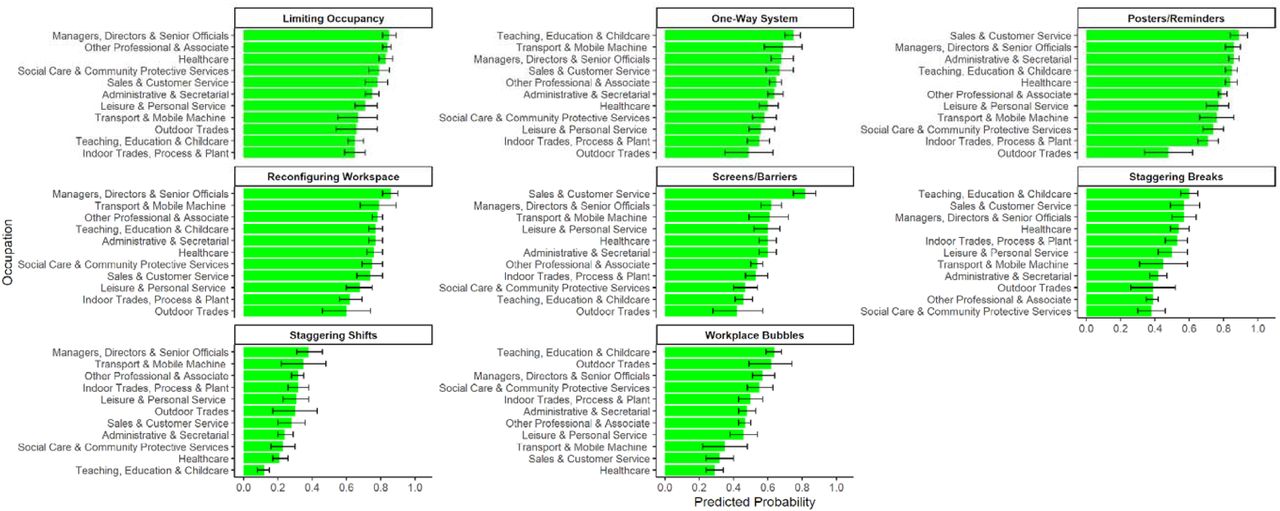
Healthcare workers had the highest predicted probabilities for several mitigations, including frequent hand and surface hygiene, wearing face coverings, and employers providing face coverings for workers and other people on worksites (Figure 2). There was a cross-occupational trend towards reduced mitigations during periods of less stringent national restrictions.
Figure 2. Strategies to Reduce Contact-Related Risk in the Workplace: Predicted probabilities by occupation
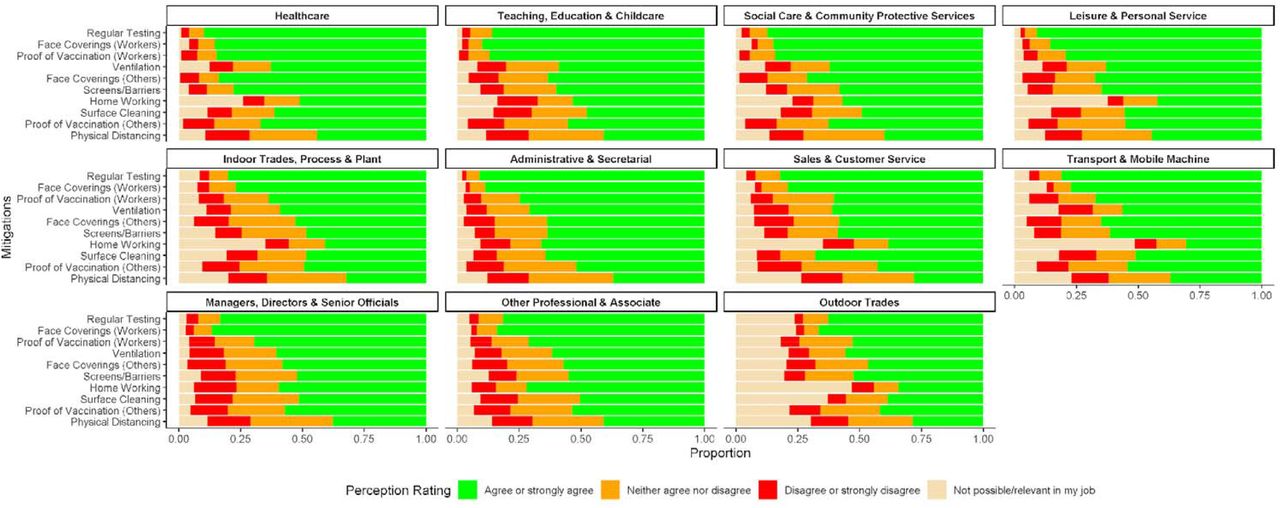
Workers’ perceptions of key work-related mitigation methods are reported by occupation in Figure 3 for late February 2022. Across all occupations ≥50% of participants agreed or strongly agreed with each measure except physical distancing. Patterns of agreement were similar across occupations, and respondents agreed or strongly agreed with the following measures in descending order: regular testing (84%), requiring face coverings for workers (84%), proof of vaccination for workers (74%), ventilation (62%), requiring face coverings for non-workers attending the worksite (62%), screens/barriers (60%), working from home (58%), surface cleaning (54%), proof of vaccination for non-workers attending the worksite (55%), and physical distancing (39%).
Figure 3. Perceptions of Work-Related Mitigation Methods in late February 2022: Proportions by occupation
This study found substantial between-occupational differences in risk-relevant workplace features and related mitigations. There was agreement that most mitigations were reasonable and worthwhile. Further investigation into the factors underlying between-occupational differences could assist pandemic planning and prevention of workplace COVID-19 transmission.
Please see this link for our full analysis.
4. Glasses and risk of COVID-19 transmission
Respiratory viruses, including SARS-CoV-2, can infect the eyes or pass into the nose via the nasolacrimal duct. The importance of transmission via the eyes is unknown but might plausibly be reduced in those who wear glasses.
19,166 Virus Watch participants responded to a monthly questionnaire on glasses and contact lens use, assessing reported frequency, the purpose of use and how likely they were to wear a mask with glasses.
Figure 4. Adjusted odds ratios and 95% confidence intervals showing association of glasses and contact use with COVID-19 infection. Adjusted for age, sex, income and occupation.

We found that after we accounted for differences in age, sex, household income and occupation, there was 15% lower risk of infection for those who reported always using glasses for general use compared to those who never wear glasses (Figure 4). The protective effect was not observed in those who strongly agreed with the statement, ‘I am less likely to wear a face covering when I have my glasses on because my glasses steam up’. We did a counterfactual analysis looking to see if there was a protective effect for participants who wore contact lenses and this analysis did not suggest a protective effect regardless of frequency of use.
Our findings suggest a moderate reduction in risk of SARS-CoV-2 infection in those who always wear glasses compared to never. Unlike other studies, our results are representative of a community setting, adjust for potential confounders and provide a counterfactual analysis with contact lenses. Our results extend the current evidence to community settings and validates proposed biological mechanisms of eye protection reducing the risk of SARS-CoV-2 transmission.